A House of Commons Select Committee established ‘to Consider the State of the Lunatic Poor in Ireland’ issued a report in 1817 which led to the passing that same year of the Establishment of Asylums for the Lunatic Poor in Ireland Act. This act was amended in 1820 and again in 1821. Cumulatively these pieces of legislation enabled the division of Ireland into a number of districts and provided that ‘all lunatic poor within every such district respectively shall be maintained and taken care of in the asylum belonging to such district’. Ireland was to become the first country in the world to have a system of publicly funded asylums for the mentally ill.
Nine asylums were built in the first programme of construction under the auspices of the Commissioners for the Erection of Lunatic Asylums. Francis Johnston, architect to the Board of Works since 1805, secured the appointment as architect to the Commission. In the delivery of the buildings, he was assisted by his cousin William Murray who succeeded as the Commission’s architect after Johnston’s death in 1829.
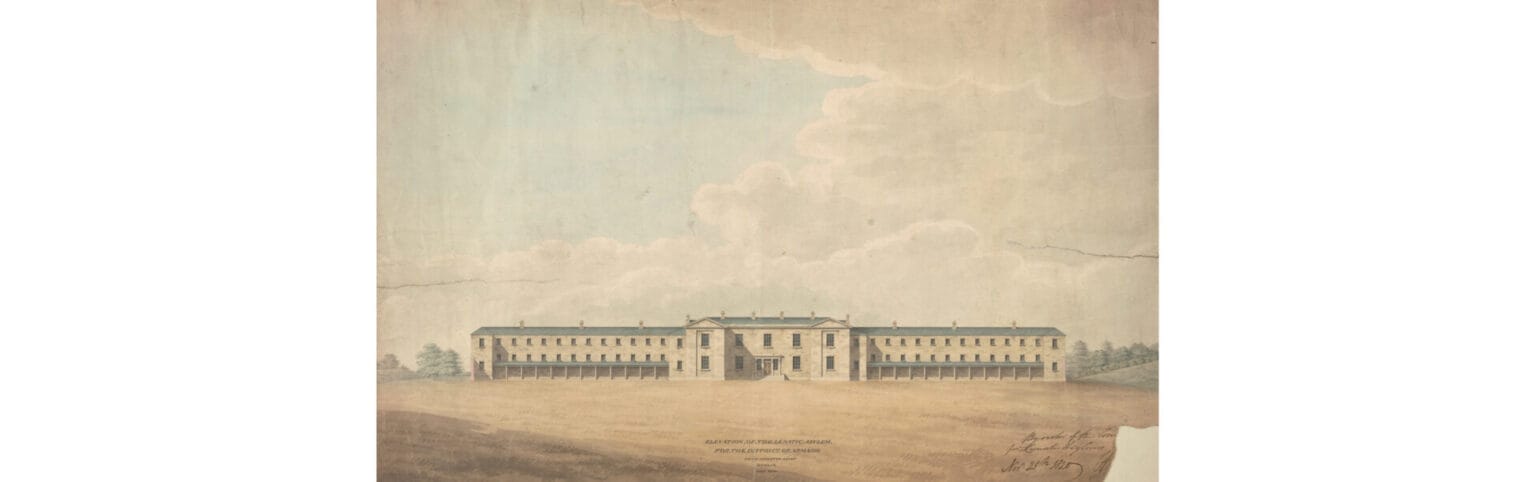
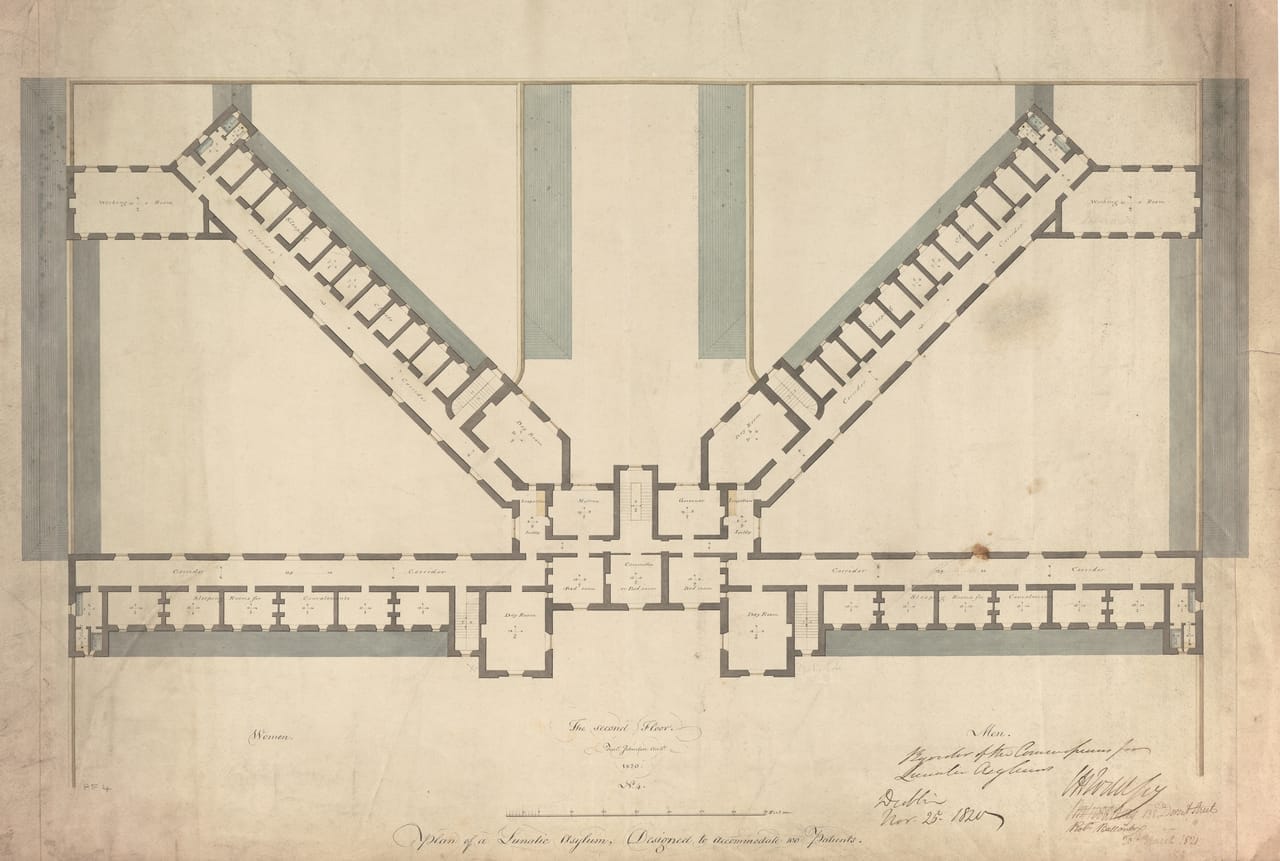
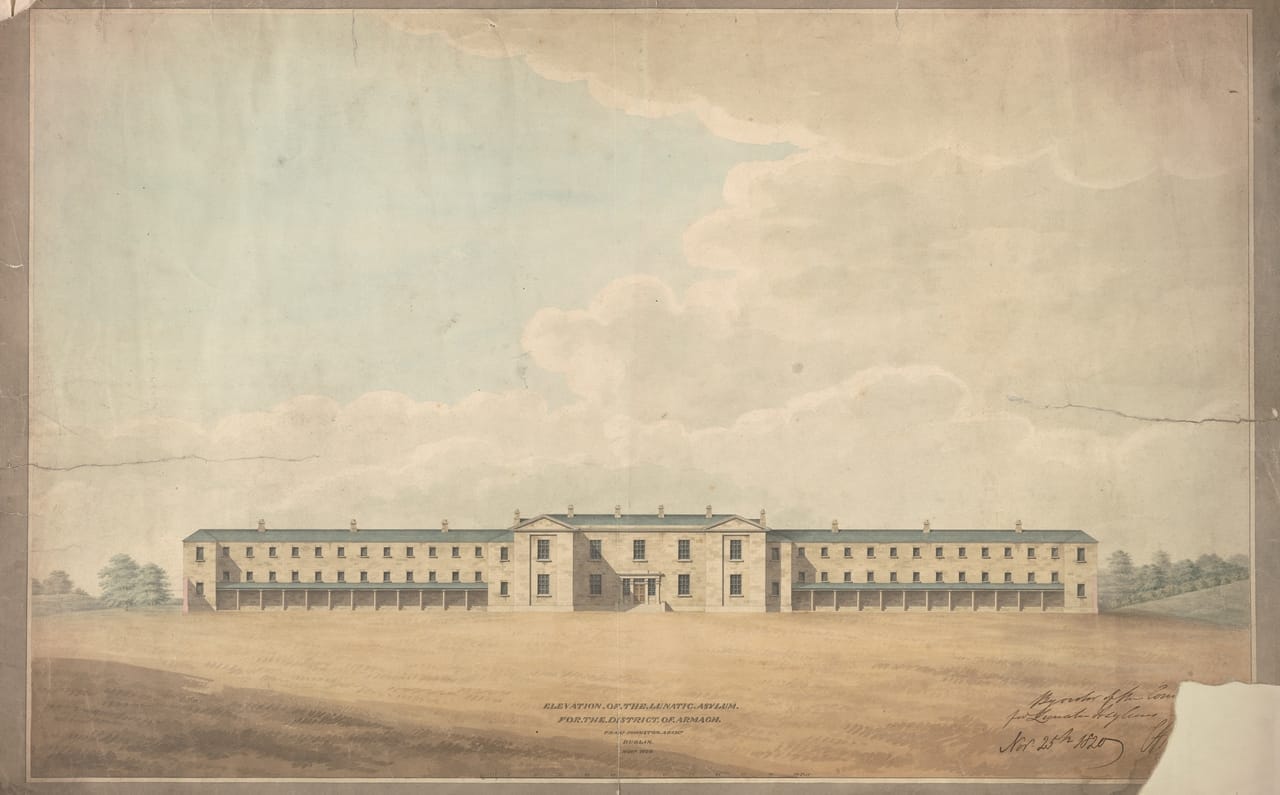
The asylum at Armagh was the first to be designed and built. As evident in this front elevation, a dignified, unadorned, Classical style was chosen as the appropriate external expression for the building. A cupola, missing from the drawing, was added during construction. The plan indicates that the architects were aware of recent innovations in the care of the mentally ill. Whereas previous asylums had resembled prisons, at Armagh the central five-bay block contained the Governor’s residence and large day-rooms. This was flanked on each side by long wings containing ‘Closets’ or cells, and larger ‘Sleeping Rooms for Convalescents’.
Armagh Asylum opened in 1825. It was the model for Limerick (1826), Belfast and Derry (both 1829), Carlow (1832), Ballinasloe, Maryborough (Portlaoise) and Waterford (all 1833), and Clonmel (1835). Much altered, it continues to serve as St Luke’s Hospital.